Case – 8
Case – 8
Diagnosis –
Occluded right distal Superficial Femoral Artery.
History –
The patient complained of right calf claudication at 100 yards which was progressively worsening for the last 4 years. There was no associated rest pain. There were no ulcers or cyanosis of the foot. Now the pain was interfering with his work because he had to walk long distances in his fields as he was a farmer. He had a stent put into the distal SFA at the level of the adductor canal but this had occluded. This was performed over 10 years ago but no records were available.
Examination –
The patient had a cooler leg than the left. There were no pulses beyond the Femoral. The power and sensation seemed good. There was no cyanosis or ulcers. He had marked varicose veins on the right leg. The left was normal. Bed-side Doppler – The right ankle signal was occluded. The brachial pressure was 120 mmHg while the ankle pressure on right side was 70 mmHg and on the left 120 mmHg
Investigations –
Bloods – 11.07.05
Hb – 14.2 mg% TLC – 10,000 /µl Platelets – 1,30,000 /µl
RBS – 109 mg% Urea – 30 mg% Createnine – 1.1 mg%
Na – 143 meq/l K – 4.3 mg% PT – 13/12 sec
PTT – 37/28 sec Bl. Gp. –
CXR – WNL
Colour Doppler Study – venous and arterial systems
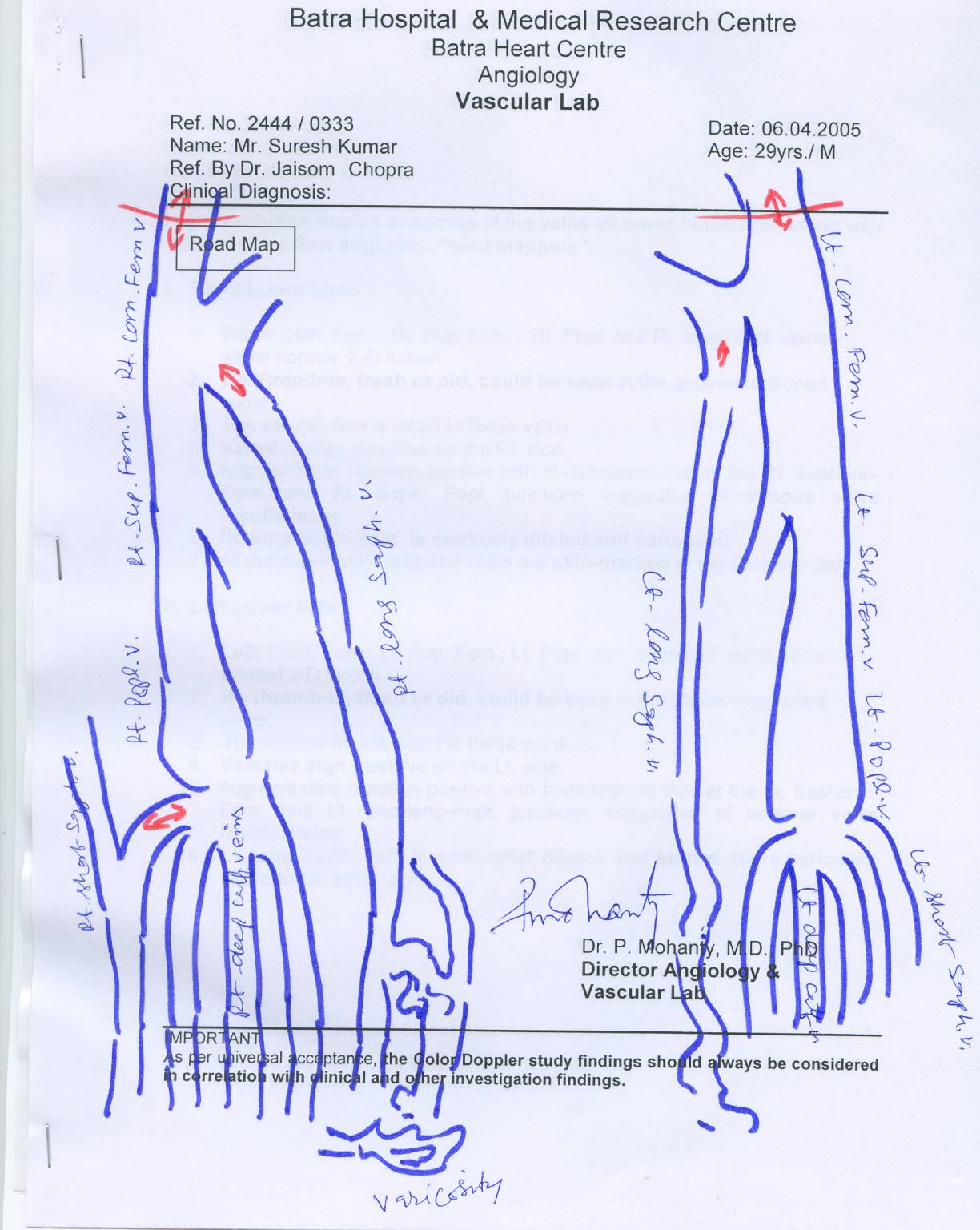
Right distal SFA total occlusion of the stent graft. There are two prominent collaterals arising proximal to the occlusion which are responsible for the circulation of the leg .
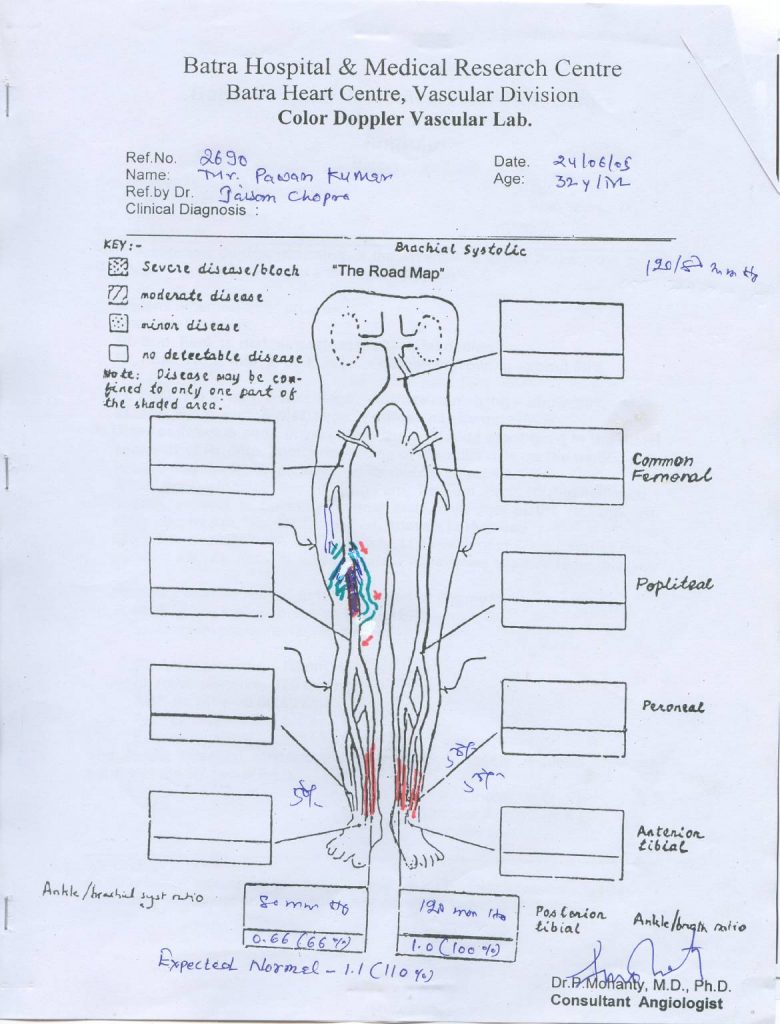
Angiogram showed minimally diseased aorta, iliacs, Right CFA and profunda but occluded distal SFA ® at the level of the adductor canal with good outflow down the right leg.
Surgery – General Anesthesia –

The SFA was exposed proximal and distal the occluded stent graft where it was soft and healthy. The proximal pulse was normal though there was no distal pulse palpable. There were marked adhesions around the stent which was not approached. The collaterals were safe-guarded. A 7 mm x 15 cm PTFE inter-ringed graft was inserted and tunneled below the deep fascia. A fogarty catheter was passed distally to be sure there was no clots and no distal occlusion. The proximal and the distal anastamosis were done using CV 6 running sutures. Haemostasis was maintained and good normal pulses were achieved in the popliteal artery.

Uneventful for the first 24 hours. Then there developed a haematoma in the thigh with occlusions of the suction drains. The pulses at the ankle were normal and strongly palpable. PT – 14/12 sec and PTT 33/28 secs. The patient was on LMWH which was stopped.
Surgery – General Ansethesia
The wound was explored and haematoma evacuated. There was a generalized ooze but no specific bleeder. Hemostasis was maintained and the wounds were once again closed over larger drains.
Post-operative period –
No obvious bleeding was found. The patient was transfused blood and mobilized.
Condition on discharge –
Pawan Kumar was apyrexial, on normal diet & mobilizing on the ward. The foot was warm with palpable pulses at the right ankle. The varicose veins were not dealt with at present and would have to be done at a later date.
Advise on discharge –
- Normal diet
- Normal activity
- Tab Augmentin 1000 mg bd for 7 days
- Cap Tramazac 1 tds if in pain otherwise SOS
- Tab Ecospirin 150 mg od
- Tab Plavix 75 mg od
- To review in the OPD in 7 days time
The patient would need varicose veins surgery on the same leg when he is fit to have it.
(Dr. JAISOM CHOPRA)
Consultant Vascular Surgeon