Case – 7
Case – 7
Diagnosis
Bilateral Varicose veins
History
The patient has had prominent varicose veins for the past 10 years and have been progressively increasing. Now there is pain in the legs and discolouration at the right ankle.

The patient is a very fit young sportsman in good general health. He is not pale. There were markedly dilated veins on the right side with dermatitis at the ankle but no ulcers. There were also visible veins on the left leg but no dermatitis.
This case is the old technique where high ligation, stripping and phlebectomies was done. Now it is obsolete and it has been over 15 years since I did it. It was a good technique and effective but very traumatic for the patient
Bed-side Doppler study
There was a strong reflux at the right SFJ and also minimal reflux at the right SPJ. On the left side there was reflux at the SFJ though not as marked as the contralateral side. Could not illicit reflux at the left SPJ.
Colour Doppler Study
Colour Doppler study of the venous system showed bilateral SF incompetence with markedly dilated, tortuous and incompetent LSV on the right side. There were incompetent perforators on the right leg with blowouts. There was also incompetence of the right SP junction.
The left leg showed incompetence of the SF junction but the LSV was not markedly dilated or tortuous. There was minimal SP incompetence.
Since there was only incompetence of the left SF junction and no dilation of the LSV it was considered inappropriate to operate on the left leg at present. Thus only the right leg was operated upon.
Surgery –– Spinal Anesthesia –
The patient had right high tie where the LSV was traced to the junction with the Femoral vein. All branches were ligated and divided. The LSV was flush doubly ligated with the FV and divided.
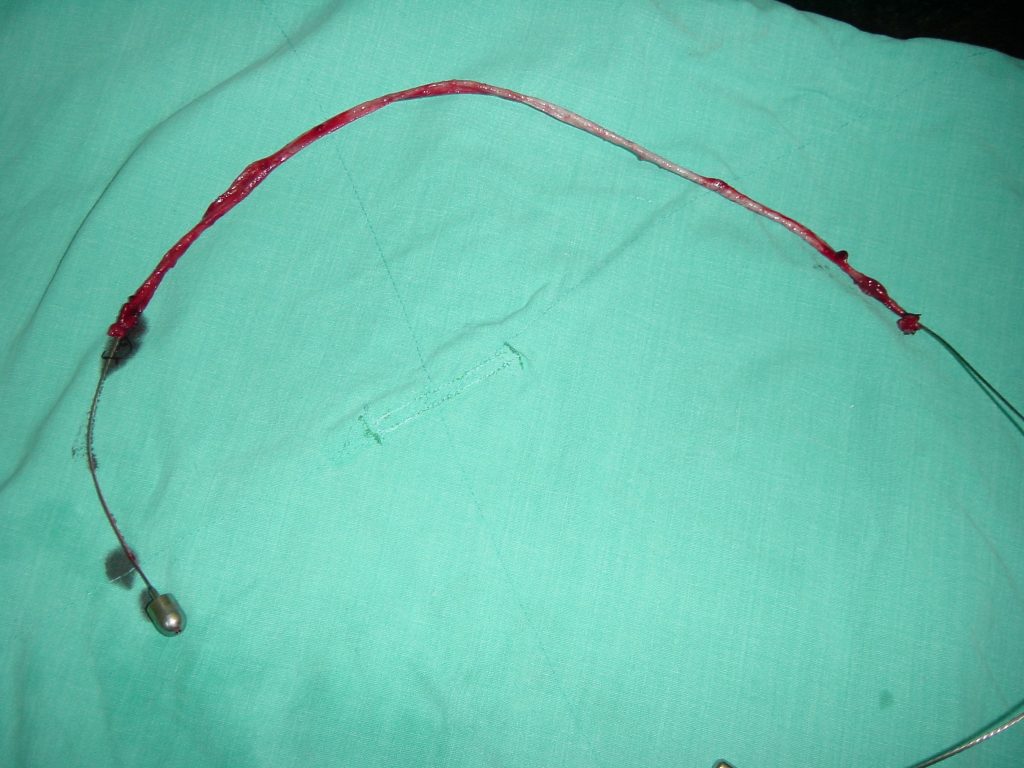
The LSV was stripped to the knee and tight bandage applied to minimize the haematoma formation.
Multiple ligations done below the knee along with two large perforators. These veins were ligated with vycril

The patient was made prone and the short Saphenous vein ligated and divided.
Post-operative period
The patient had pain main in the back at the site of the spinal anesthesia. He was on bed rest for the first 24 hours and then mobilized.
Condition on discharge
The patient is mobilizing on the ward and on normal diet. He had some pain understandably, but this should settle fast. There are no haematomas.
Advise on discharge
- Normal diet and plenty of fluids orally
- Normal activity with long walks
- Tab Distaclor 750 mg bd for 7 days
- Cap Tramazac 1 tds for days and then SOS, if in pain
- Tab Nucoxia 1 at bed time, if in pain
- To keep crape bandage on till Monday and retighten it if it becomes loose
- To attend OPD on Monday 11.04.05.
(Dr. JAISOM CHOPRA)
Consultant Vascular Surgeon